Get Easy Health Digest™ in your inbox and don’t miss a thing when you subscribe today. Plus, get the free bonus report, Mother Nature’s Tips, Tricks and Remedies for Cholesterol, Blood Pressure & Blood Sugar as my way of saying welcome to the community!






20+ medications that affect your thyroid

Thyroid hormone balancing is confusing for mainstream doctors including endocrinologists (but they may not admit it).
That’s because they use only lab tests such as the Thyroid Stimulating Hormone (TSH), Triiodothyronine (T3) and Thyroxine (T4) to evaluate your thyroid. The problem with that is there are many medications that affect your thyroid hormone and confound the interpretation of standard thyroid tests.
Let’s look at these medications and why you must correlate signs and symptoms with lab tests to properly balance thyroid hormone…
Drugs that adversely affect the thyroid
There are important steps in how thyroid hormone is synthesized, released, transported, absorbed, controlled and metabolized. All of these are susceptible to interactions with medications. Your doctor may not have considered drug-induced thyroid dysfunction when interpreting your thyroid level blood tests.
The list of medications known to throw off your thyroid hormone tests is increasing. Let’s begin with the over-the-counter medications you probably never thought could do this.
Several categories of medications will artificially drop the TSH (thyrotropin) level, but not change the circulating T4 level:
- Metformin which is very commonly prescribed to reverse pre-diabetes and to help lose weight.
- Prednisone (all glucocorticoids) commonly used for many acute (asthma, allergic reactions, etc.) and chronic inflammatory conditions.
- Dopamine agonists (Mirapex, Parlodel, Requip) commonly used for various conditions such as Parkinson’s disease, restless legs, and to slow breast milk production after baby delivery.
- Somatostatin analogues (e.g. Octreotide) to treat acromegaly.
Low TSH (thyrotropin) level with a normal free T4 level may be confused with subclinical hyperthyroidism, prompting incorrect interpretation and treatment.
Some interfere with thyroid hormone activation, metabolism, and excretion:
- Prednisone (again!) which is used for many conditions, inhibits conversion of T4to the more active thyroid hormone T3. Propranolol at high doses acts similarly.
- Chemotherapy medicines such as the synthetic retinoid bexarotene (Targretin) used to treat cutaneous T cell lymphoma. It rapidly and profoundly suppresses TSH (thyrotropin) in 40 – 70% of treated patients. Normal recovery occurs within weeks after drug discontinuation. Mitotane (Lysodren) used for adrenal gland carcinoma and Cushing’s syndrome. It causes hypothyroidism in most patients who take it.
- Seizure control medicines such as phenobarbital, phenytoin, carbamazepine, and rifampin sometimes cause the need to increase thyroid hormone dosing.
- Salsalate (an NSAID) has a similar effect as seizure control medicines listed above.
- Heparin displaces T4 and T3 from their binding proteins; this causes a spuriously high value.

«SPONSORED»
Medications that affect thyroid hormone synthesis or release include:
- Amiodarone (for heart rhythm control) is 37.3% iodine by weight and induces hypothyroidism in susceptible patients, and hyperthyroidism in others.
- Sources of excess iodine include CT contrast agents, topical povidone, over-the-counter expectorants, vaginal douches, and kelp.
- Lithium (for bipolar) use causes goiter and hypothyroidism by decreasing thyroid hormone release
Several medications increase thyroxine-binding globulin:
- Estrogen by oral route increases in protein binding of T4. Transdermal estradiol has minimal effects on thyroxine-binding and is always recommended over oral dosing as this circumvents the first-pass effect on the liver.
- Selective estrogen-receptor modulators
- Methadone
Several medications reduce this protein:
- Androgens
- Glucocorticoids (prednisone)
- Niacin
GI absorption of thyroid hormone pills is very common. Approximately 60 to 80% of thyroid hormone T4 is absorbed within 2 – 4 hours after ingestion on an empty stomach. Here are medicines that will interfere with thyroid hormone absorption:
- Proton-pump inhibitors (PPIs) such as Nexium, Protonix, Prilosec generally will lower absorption and cause a need to increase thyroid dosing.
- Iron (ferrous sulfate)
- Calcium carbonate
- Aluminum hydroxide
- Sucralfate (Carafate)
- Bile acid sequestrants (e,g, Cholestyramine, Colestipol)
- Raloxifene (Evista) to prevent osteoporosis
Therefore, take thyroid hormone four hours before or after ingesting any of these; best on an empty stomach.
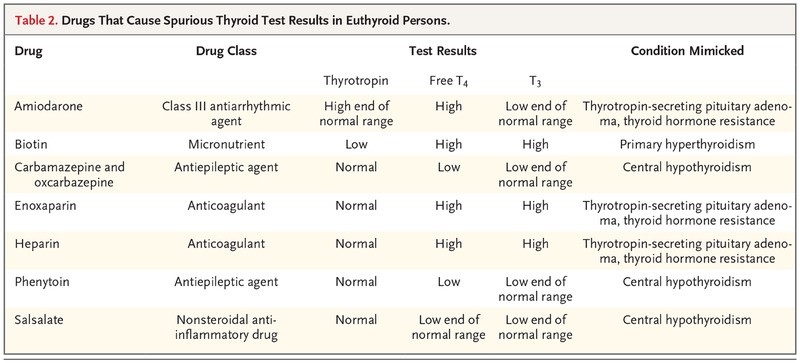
Medications causing abnormal thyroid tests in otherwise normal thyroid (euthyroid) patients
For a summary of medications causing abnormal thyroid tests in otherwise normal thyroid (euthyroid) patients, take a look at table 2 below.
Table 2
Sources:
- Lupoli R, Di Minno A, Tortora A, Ambrosino P, Lupoli GA, Di Minno MN. Effects of treatment with metformin on TSH levels: a meta-analysis of literature studies — J Clin Endocrinol Metab 2014;99:E143-E148
- Beck-Peccoz P, Rodari G, Giavoli C, Lania A. Central hypothyroidism — a neglected thyroid disorder — Nat Rev Endocrinol 2017;13:588-598
- Duvic M, Martin AG, Kim Y, et al. Phase 2 and 3 clinical trial of oral bexarotene (Targretin capsules) for the treatment of refractory or persistent early-stage cutaneous T-cell lymphoma — Arch Dermatol 2001;137:581-593
- Curran PG, DeGroot LJ. The effect of hepatic enzyme-inducing drugs on thyroid hormones and the thyroid gland — Endocr Rev 1991;12:135-150
- McConnell RJ. Abnormal thyroid function test results in patients taking salsalate — JAMA 1992;267:1242-1243
- Mendel CM, Frost PH, Kunitake ST, Cavalieri RR. Mechanism of the heparin-induced increase in the concentration of free thyroxine in plasma — J Clin Endocrinol Metab 1987;65:1259-1264
- Ross DS, Burch HB, Cooper DS, et al. 2016 American Thyroid Association guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis — Thyroid 2016;26:1343-1421
- Perrild H, Hegedüs L, Baastrup PC, Kayser L, Kastberg S. Thyroid function and ultrasonically determined thyroid size in patients receiving long-term lithium treatment — Am J Psychiatry 1990;147:1518-1521
- Arafah BM. Increased need for thyroxine in women with hypothyroidism during estrogen therapy — N Engl J Med 2001;344:1743-1749
- Shifren JL, Desindes S, McIlwain M, Doros G, Mazer NA. A randomized, open-label, crossover study comparing the effects of oral versus transdermal estrogen therapy on serum androgens, thyroid hormones, and adrenal hormones in naturally menopausal women — Menopause 2007;14:985-994
- Sachmechi I, Reich DM, Aninyei M, Wibowo F, Gupta G, Kim PJ. Effect of proton pump inhibitors on serum thyroid-stimulating hormone level in euthyroid patients treated with levothyroxine for hypothyroidism — Endocr Pract 2007;13:345-349
- Drug Effects on the Thyroid — New England Journal of Medicine

By Dr. Michael Cutler



«SPONSORED»